

 One of the most common interventional therapeutic procedures on the spine is facet block (injection into the intervertebral joints of the cervical, thoracical and lumbar spine).
One of the most common interventional therapeutic procedures on the spine is facet block (injection into the intervertebral joints of the cervical, thoracical and lumbar spine).
The images illustrate the anatomical conditions at the lumbar spine in transition to the pelvis using a skeleton model (beige: intervertebral discs, creme: vertebral body with spinous and transverse processes and intervertebral joints, yellow: in the middle spinal channel on both sides spinal nerves, cannula with blue head Kopf in the intervertebral joint of lumbar vertebral bodies 4 and 5, on the right red. schematic representation of a herniated disc
It is used especially for treatment of the so-called facet syndrome. As a rule this is associated with an arthrosis of the intervertebral joints (possible from the age of 30) and the and the associated muscular tensions in the back area.
The capsules of the intervertebral joints have a very good nerve supply, so that the slightest changes in the joints and their environment can be registered and felt painfully. The facet syndrome shows different manifestations and then has to be differentiated from other disease patterns.
Locally limited pain, e.g. with lumbago, can be found here as well as radiating pain in the sense of lumboischialgia, but also dysesthesia (numb feeling) and tingling paresthesia (running ants).
So-called pseudoradicular pain must sometimes be distinguished from real radiculopathies (pain radiation of the nerves) in herniated disc-related nerve root compression.
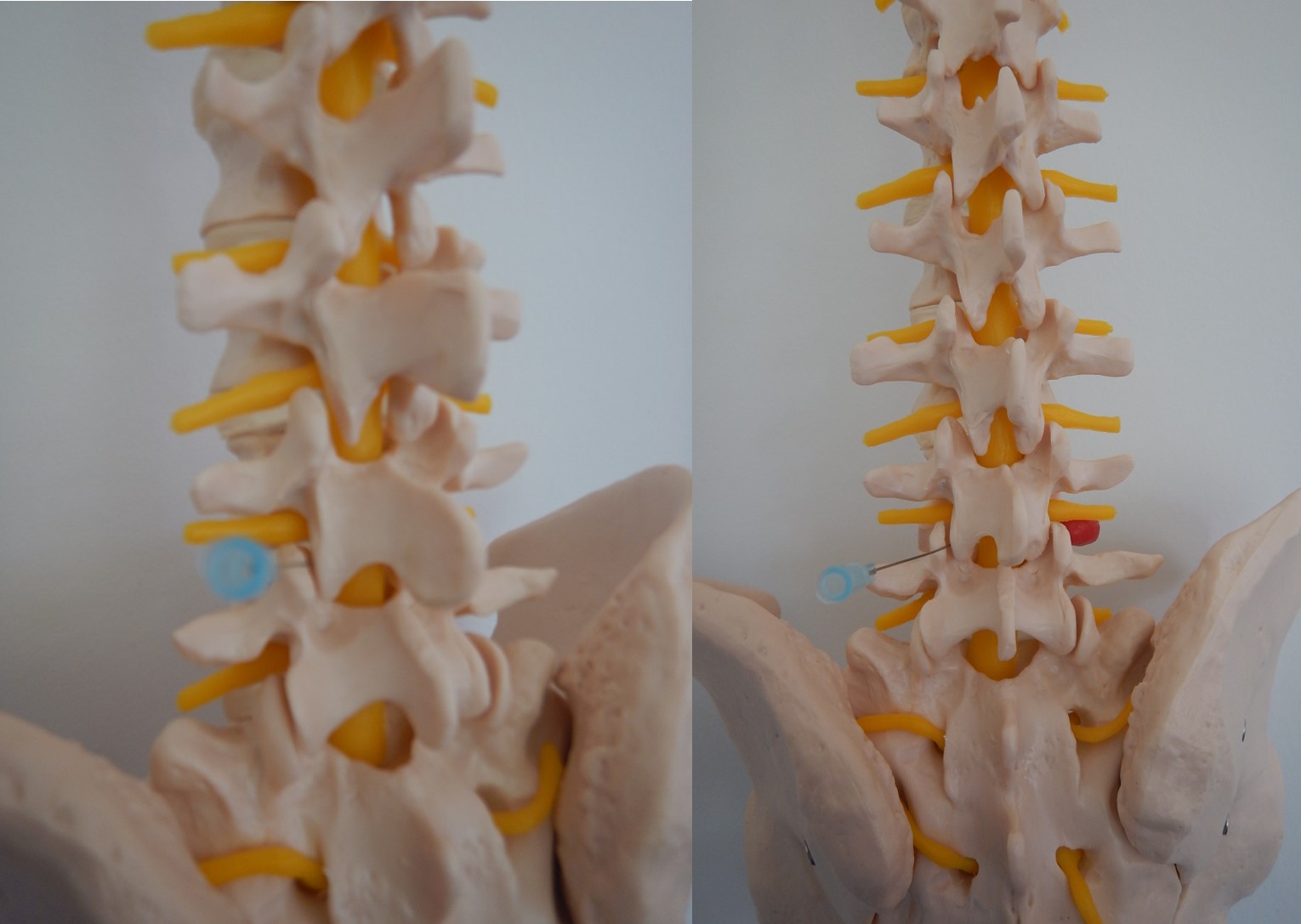 The facet blockade involves pain treatment of the small vertebral joints (facet joints) and their surrounding tissue; using an imaging procedure such as the C-arm, computer tomography (CT), but also under ultrasound control, drugs are injected precisely into the facet joints (here a schematic representation of an injection into the intervertebral joint 4/5).
The facet blockade involves pain treatment of the small vertebral joints (facet joints) and their surrounding tissue; using an imaging procedure such as the C-arm, computer tomography (CT), but also under ultrasound control, drugs are injected precisely into the facet joints (here a schematic representation of an injection into the intervertebral joint 4/5).
A local anaesthetic is used to relieve nerve pain by reducing the sensitivity of the nerve supply to pain sensations. First of all, a local anaesthetic with a rapid onset and shorter duration of action is used to assess the desired effect on the one hand and to limit any possible side effects temporarily on the other hand.
If this first infiltration shows the desired effect without side effects, a new infiltration with a longer effective local anaesthetic can be carried out after at least one week.
Adding drugs like cortisone, but also Traumeel and/or Acidum formicicum prolongs the duration and improves the quality of the facet block.
In individual cases, after the 1st infiltration there is already a permanent reduction in pain, ideally even freedom from pain. Usually I plan 2-3 injections in a sequence, for more persistent complaints 4-5.
If the infiltrations result in a reduction of pain without permanent complete freedom from symptoms, a combination with other procedures such as periradicular therapy (injection to one or more nerve roots) and/or ablative (sclerosing) procedures by heat exposure (radiofrequency) can make medical sense.
In case of repeated complaints and after a successful infiltration treatment, I recommend the TENS (transcutaneous electrical nerve stimulation) treatment, which can be carried out on your own with a TENS device after appropriate adjustment and instruction. This recommendation is based on the positive correlation between therapeutic local anaesthesia and TENS (Wall and McKenzie, 1965).